Introduction
Sporotrichosis is a mycotic disease caused by the ubiquitous dimorphic fungus Sporothrix schenckii, which infects humans, usually through cutaneous trauma with dead plant parts, wood, or thorns [1]. However, animals, including cats, also suffer from sporotrichosis, which can be a source of human infection [2]. Infection through the skin most frequently leads to the classic form of lymphocutaneous sporotrichosis, where a pustule or papule forms a few weeks after a minor injury, followed by a nodule or ulcer. Such a lesion may resolve spontaneously, but new subsequent lesions may appear along the course of the lymphatic vessels [3]. The disseminated cutaneous form of sporotrichosis presents mainly in immunosuppressed people, e.g. human immunodeficiency virus-positive patients. Potential risk factors for the complicated course of the disease also include other comorbidities such as diabetes mellitus, chronic alcoholism, steroid treatment, hematologic malignancies and organ transplantation [4].
A leg ulcer is full-thickness skin loss on the leg or foot of numerous etiologies, e.g. venous or arterial insufficiency, diabetes, skin cancer, vasculitis, or infections [5-13]. However, one should include rarer causes of limb ulcerations in the differential diagnosis, especially in patients with immunosuppression or multiple morbidities, as well as in cases of lesions not responding to various treatments. We present a case report of an unusual coincidence of sporotrichosis and late latent syphilis diagnosed in a patient with disseminated leg ulcerations, accompanied by a literature review. As indicated by available reports, we aimed to analyze the probable causes of sporotrichosis in immunocompromised patients and those with other comorbidities.
Case report
A 49-year-old man presented to the Department of Dermatology with diffuse, painful, itchy ulcerations on the lower limbs, which he began developing approximately four weeks after being scratched by a stray cat. Four lesions were observed around the left ankle (three on the lateral side and one on the medial side of the ankle) and one on the medial part of the right thigh (Fig. 1). The first lesion appeared on the right tibia precisely at the site of the cat scratch and measured about 5 cm in diameter. Subsequently, other lesions almost simultaneously emerged around the left ankle and thigh approximately two weeks after the first one. The most recent lesion was located on the left buttock. Only the first lesion on the right tibia was situated at the site of the cat scratch; the other lesions were not in contact with the animal’s claw, raising suspicion of potential hematogenous spread or autoinoculation.
Fig. 1
Lesions on the patient’s lower legs: on the right lower leg (in the place of the primary cat scratch), around the left ankle (lateral and medial side), and on the medial part of the thigh

The patient had type 2 diabetes mellitus treated with dapagliflozin, sitagliptin, and gliclazide. Other medical history was unremarkable. Before admission to the Department of Dermatology, the treatment of the skin lesions included topical clobetasol, gentamicin, betamethasone, oral clemastine, erythromycin, and methylprednisolone. Still, it resulted only in a slight improvement.
During the hospitalization, a deep tissue biopsy and a swab from the biopsy wound were taken from the ulcer on the right lower leg for both mycological tests and microbiological culture. The biopsy for the histopathological examination was taken from the ulcer on the left thigh. Direct immunofluorescence (DIF) from the lesion on the left buttock was also performed, and the results were negative. No deposits were found that were characteristic of autoimmune bullous diseases. A complete blood count (CBC) did not show any deviance (a hemoglobin concentration [Hb] of 16.5 g/dl, hematocrit [HCT] of 47.2%, leukocyte count of 9,340/µl with 61.3% neutrophils, 27.4% lymphocytes, 8.6% monocytes, 0.6% eosinophils, and 0.7% basophils, and a platelet count of 257,000/µl). The laboratory test results indicated an increased fasting glucose level upon admission (227 mg/dl), elevated postprandial glucose levels (peaking at 282 mg/dl), and raised glycated hemoglobin (9.2%), heightening suspicion of susceptibility to infection. Over 500 mg/dl of glucose was noted in the routine urinalysis. Hypercholesterolemia with hypertriglyceridemia was also observed. An ELISA panel for autoimmune blistering dermatoses was negative. The antinuclear antibodies (ANA) measured by IIF (indirect immunofluorescence) were present in 1 : 160 titers.
Mycological analysis of the swab from the biopsy wound revealed the presence of mycelial hyphae (Fig. 2), which led to the initial diagnosis of sporotrichosis. The growth of Sporothrix spp. was later confirmed in the culture from the deep tissue biopsy (Fig. 3).
Fig. 2
Mycelial hyphae found in the swab from the deep biopsy tissue from the lesion on the right lower leg, primarily scratched by a stray cat
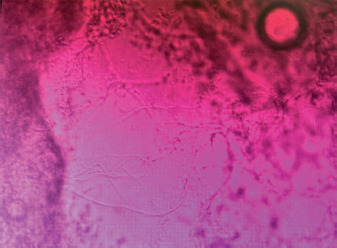
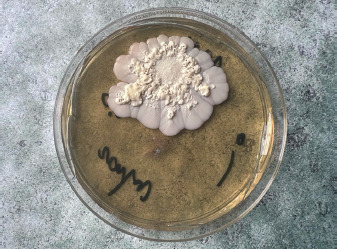
Fig. 3
The culture from the deep tissue biopsy from the lesion on the right lower leg (Sporothrix spp.)
Our Department of Dermatology routinely performs a screening test for Treponema pallidum antibodies for every admitted patient. Unexpectedly, the results of the test returned positive for the reported patient. Following that, we found a positive titer of Treponema pallidum hemagglutination assay (TPHA) in the blood of 1 : 320, and rapid plasma reagin (RPR) was negative. These examinations were repeated, and identical results were achieved. The patient was neither treated for syphilis nor did he suspect the infection throughout his life. When asked about the potential symptoms of syphilis, such as genital ulcers, rashes, regional or general lymphadenopathy, hair loss, and neurological disorders, the patient denied experiencing any of these. He denied having unprotected and risky sexual contact for the past two years but could not dismiss such occurrences from earlier periods, all heterosexual. We diagnosed late latent syphilis. Moreover, the histopathological test revealed that the biopsy from the lesion on the left thigh might match the syphilitic exanthem with dermatitis (Fig. 4A, B).
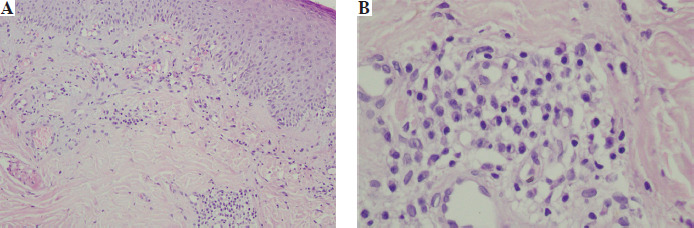
Fig. 4
A, B) The histopathological image from the biopsy of the lesion on the left thigh. The epidermis moderately thickened with slight hyperkeratosis, thickening of the granular layer, and moderate edema. The superficial and deep plexus vessels dilated, surrounded by small infiltrates dominated by plasma cells. No signs of sporotrichosis. Possible correspondence with syphilitic exanthem with the coexistence of eczema
The medical history of this patient excluded organ transplantation or the use of immunosuppressive medication now or in the past. The results of the rapid human immunodeficiency virus (HIV) test, hepatitis B surface antigen (HBsAg), and hepatitis C virus antibody (anti-HCV) were non-reactive. The titer of antinuclear antibodies (ANA) was 1 : 160, with no detected specificity.
Following CDC guidelines, in the case of two positive treponemal tests (in the reported patient, TPHA and Treponema pallidum ELISA IgG antibodies), if no medical history or physical examination suggests a recent infection, individuals who have not received prior treatment should be managed for syphilis of unknown duration or late latent stage syphilis [14]. Consequently, the patient was treated for late latent syphilis with 2.4 million units of benzathine penicillin administered intramuscularly three times at weekly intervals. The patient was also treated for sporotrichosis with itraconazole prescribed at a dosage of 200 mg orally twice daily for two months. The man was also referred for diabetological consultations. During ophthalmological, neurological, and laryngological consultations, no abnormalities were observed. After two months, the dermatological condition significantly improved, and the ulcers mostly healed.
Discussion
Epidemiology and clinical manifestation
Sporotrichosis has been reported worldwide; however, most cases have been described in tropical and subtropical areas of Central and South America, Asia and Africa [4]. Several occupational groups are especially susceptible to the disease. Gardeners, farmers, and miners are more commonly affected. The disease may be caused in children by playing in farm fields or dusty floors. This infection is classified as an implantation mycosis, as it is typically transmitted via trauma by introducing a fungus into subcutaneous tissues. The exact prevalence of sporotrichosis is unknown due to the absence of an obligation to report the disease [1, 15].
While trauma from contaminated plants or soil is commonly reported, infection can also arise from zoonotic transmission, primarily through scratches and bites from infected cats [16]. Other animals, including dogs, rats, squirrels, armadillos, and birds, may also suffer from sporotrichosis. Zoonotic transmission is predominantly associated with dogs and cats, particularly domestic cats, which serve as primary reservoirs. Positive cultures have been identified in samples from their skin lesions, nasal cavity, oral cavity, and nails. This supports the hypothesis that transmission can occur through scratches or bites from these animals, as well as through contact with secretions containing infectious microorganisms. Cats can remain infected for several months, with some showing no symptoms, acting as a reservoir for the fungus [16-18]. Zoonotic transmission was the most likely cause of the Sporothrix infection in the patient reported in our paper.
Cutaneous and extracutaneous forms of sporotrichosis are distinguished. The disease is usually limited to the skin and subcutaneous tissue [19]. Four clinical forms of the disease have been described: lymphocutaneous (LC), fixed cutaneous (FC), disseminated cutaneous, and extracutaneous [1]. LC sporotrichosis is the most common form, characterized by linearly spread, painful and itchy nodules that occur mainly on the extremities and facial skin [20]. The later stage may result in ulceration of the lesion and fistula formation with purulent discharge [21]. FC forms are characterized by a single asymptomatic papillary or squamous lesion at the area of inoculation [20]. The disseminated cutaneous form represents a rare form of sporotrichosis, with lesions occurring at various anatomic locations, possibly due to spread from a single lesion through the bloodstream or multiple inoculations. The extracutaneous form is more common in immunosuppressed patients. Osteoarthritis is the most frequent form, usually involving the knee, wrist, elbow and ankle joints, and manifested by tenosynovitis and joint effusion. Skin lesions are rarely present [22]. The disease can also affect the mucous membranes, eyes, lungs, liver, kidneys, central nervous system, and genital organs [1]. Central nervous system involvement is most often associated with AIDS and is one of the most serious complications of the disease. Manifestations of central nervous system involvement include meningoencephalitis and hydrocephalus, presenting, among other things, with headache, neck stiffness, vomiting, and fever [23].
Diagnosis and treatment
Diagnosis of sporotrichosis is based on the clinical picture, laboratory tests, and epidemiological data. Diagnostics include culture setting, cytopathological examination, histopathological examination, molecular, serological, and immunohistochemical methods [24]. The primary method is the isolation of Sporothrix species and identification based on morphological parameters. However, this method does not apply to atypical, extracutaneous forms. The most common isolation is from clinical samples such as secretions, abscess aspirates, and biopsied tissue fragments [4]. Cultures are carried out on agar medium at 25°C. Histopathological examination of cutaneous sporotrichosis is characterized by epidermal hyperplasia, central ulceration, acanthosis, and peripheral hyperkeratosis. The histopathological picture of sporotrichosis is reminiscent of many other granulomatous diseases, including tuberculosis and cutaneous sarcoidosis [20]. In immunocompetent patients, direct mycological and histopathological examinations show low sensitivity, while in immunocompromised patients, especially those with AIDS, these methods show much higher sensitivity [4]. In immunosuppressed patients, direct microscopic examination is more often positive; direct microscopic examination differs from the culture in its lower sensitivity and specificity. Treatment is selected based on the clinical form of the disease, immune status and species of Sporothrix [21]. The drug of choice in patients with the cutaneous or lymphocutaneous form is itraconazole [22]. The daily dose of itraconazole is 100-400 mg and depends on the severity of the disease and the patient’s immune status. Therapy usually lasts 3-6 months; it is necessary to continue treatment for 4-6 weeks after complete clinical remission. In immuno- compromised patients, suppressive treatment for life is often needed [24]. The therapy can be applied continuously or in a pulsed manner [22]. Itraconazole has several drug interactions; if its use is contraindicated, terbinafine is the second-line therapy for lymphocutaneous and cutaneous sporotrichosis [4]. Terbinafine is recommended in the elderly because it has fewer drug interactions and is not influenced by gastric pH [25]. In lymphocutaneous and fixed cutaneous sporotrichosis, the oral saturated solution of potassium iodide (SSKI) is also indicated. It is used initially in a dose of 5 drops 3 times daily; the dose is increased daily by five drops to a maximum of 30-40 drops. SSKI is widely used due to its low cost but may be toxic in patients with renal failure and those treated with angiotensin-converting enzyme inhibitors and potassium-sparing diuretics [20]. In life-threatening cases, in the disseminated form, systemic, pulmonary, meningeal, and osteoarticular forms, amphotericin B is used initially; after clinical improvement, it is recommended that treatment be switched to itraconazole [20, 24, 26]. Treatment of the localized form is usually adequate, but the response to treatment is substantially worse in extracutaneous forms such as osteoarticular or disseminated [4, 27].
Immunopathogenesis of sporotrichosis
Different signaling pathways and immune receptors are involved in Sporothrix spp. recognition, possibly depending on the route of infection and the specific species [4]. In the cutaneous form, the most common route of infection is through the damaged skin. After incubation with Sporothrix schenckii, the primary lesion is formed as a chancre. This process activates an innate immune response involving CD4+ lymphocytes, macrophages, dendritic cells, and neutrophils. Sporothrix schenckii transforms into yeast forms to survive in the human body [23, 24, 28]. Macrophages play a key role in the host inflammatory response, phagocytosing invasive forms of the fungus and presenting antigens to T lymphocytes. This process stimulates the production of pro-inflammatory cytokines such as interleukin (IL)-β, IL-4, IL-6, and tumor necrosis factor α (TNF-α). These cytokines, especially TNF-α, trigger macrophages to produce nitric oxide (NO), which is toxic to the fungus [28]. An important role is played by the dectin-1 cell receptor, which recognizes fungal components such as β-glucan and α-mannan and stimulates the Th-17 response. Another essential receptor is TLR2, which promotes phagocytosis of fungal components by stimulating cytokine and NO production. Dendritic cells modulate the immune response depending on the amount of antigen. At higher concentrations, antigens lead to the formation of Th-1 and Th-17 lymphocytes [29]. Mast cells may also participate in the immune response, but their release of histamine may have a more detrimental effect on the host than eliminating the fungus [4]. To develop sporotrichosis, the fungus must avoid the immune response and cell death caused by reactive oxygen species (ROS). Ergosterol in the fungus’s cell membrane reacts with hydrogen peroxide to form ergosterol peroxide, which protects the fungus from the body’s immune response [28]. Some studies suggest that melanin expression can also protect strains of Sporothrix schenckii from phagocytosis and oxidative stress [4].
Sporotrichosis in HIV-infected patients
It has been shown that in HIV-infected patients with sporotrichosis, the skin is most often involved. Still, multiple organs are frequently involved, possibly related to coexisting immunosuppression [30]. HIV co-infection modifies the clinical course and severity of sporotrichosis depending on the degree of immunosuppression [4]. Bone and visceral involvement may occur in AIDS patients [10]. HIV co-infection may modify the course of the disease, causing a higher fungal load; therefore, disseminated cutaneous and systemic sporotrichosis is more common in immunodeficient patients with HIV [31]. The drug of choice in patients with HIV is amphotericin B, used as an initial treatment, followed by maintenance treatment with itraconazole. Multiple and extensive skin lesions characterize sporotrichosis in HIV-positive patients [20, 22]. It has been shown that central nervous system involvement is often associated with AIDS due to the possibility of hematogenous transmission and crossing the blood-brain barrier, and dangerous complications such as subacute or chronic meningitis can occur. Increased severity of sporotrichosis is generally associated with lower levels of CD4+ cells. The literature indicates that a CD4+ cell count below 200 cells/µl is a factor in developing systemic sporotrichosis [32]. Special caution in the treatment with itraconazole in the case of concomitant AIDS is required in patients taking antiretroviral therapy, e.g. efavirenz, ritonavir, and darunavir, due to numerous drug interactions [4]. Immune reconstitution inflammatory syndrome occurs in approximately 7% of patients on antiretroviral therapy [23].
Sporotrichosis and other comorbidities – diabetes mellitus, alcohol dependence, patients after transplantations, and other immunosuppressive conditions
Diabetic patients have a higher risk of developing sporotrichosis due to impaired immunity. Several mechanisms that weaken the immune response have been described in people with diabetes mellitus. Decreased activity of cytokines such as IL-2, IL-6, IL-10, and IL-22, reduced chemotactic, phagocytic, and adhesion activity of neutrophils and monocytes, and increased cellular susceptibility to oxidative stress have been observed. This increases the risk of dissemination via the bloodstream and the development of extracutaneous sporotrichosis [28].
Alcoholism is recognized as a risk factor for sporotrichosis [4]. Chronic alcohol abuse can cause leukopenia and impaired T-cell ability to respond to pathogens [33]. Moreover, reduced levels of TNF and IL-β are observed in patients who abuse alcohol, which leads to decreased cellular immunity and impaired macrophage function [34].
Patients with AIDS with a reduced CD4+ cell count, as well as patients after transplantation, undergoing chemotherapy, glucocorticoid therapy or taking TNF antagonists, are at risk of widespread disseminated systemic sporotrichosis. It often manifests as fungemia, visceral involvement, and diffuse cutaneous or multifocal extracutaneous form. Relapses most commonly occur in immunocompromised patients [27]. Renal transplant patients are at greater risk of opportunistic infections due to immunosuppressive therapy [35]. 6% of infections in transplant patients are opportunistic fungal infections [36]. Among renal transplant patients, sporotrichosis occurs mainly in patients not using antifungal prophylaxis. Itraconazole therapy may lead to an increase in calcineurin inhibitor levels; therefore, such patients require an appropriate dosage based on the serum concentration of the drug [35, 37].
Sporotrichosis and syphilis
Skin lesions during sporotrichosis may resemble other disease entities such as tuberculosis, syphilis, cryptococcosis, and other fungal and bacterial infections [38]. Mazori et al. described a case of secondary syphilis with a sporotrichoid pattern where the skin lesions were localized along the lymphatic drainage, involving the retroauricular, posterior cervical, and occipital lymph nodes. In the course of secondary syphilis, the spread is by the blood and lymphatic route, which explains this distribution of skin lesions. The authors emphasize the importance of localizing sporotrichoid lesions in the differential diagnosis. In the case of secondary syphilis, cutaneous lesions occur in the head and neck region, whereas in other sporotrichoid diseases, they usually occur in the lower limb region [39], as in the case reported in our article. This case presents a possible coexistence of sporotrichosis and sporotrichoid pattern of lesions in secondary syphilis, which underlines the importance of adequate diagnostic methods such as suitable laboratory tests and mycological cultures.
Importantly, such coincidences of diseases presenting with skin lesions could appear more frequently in the future, especially including syphilis. Recent reports indicate that syphilis incidence has significantly increased in many continents and countries, both before and after the COVID-19 pandemic [40-42]. Syphilis, often called the great imitator, has various possible mucocutaneous presentations, for instance, nodular, lichenoid, annular, or bullous, particularly in patients with immunodeficiencies [43-46]. The literature includes reports of unique cases, such as a patient newly diagnosed with type 2 diabetes mellitus who experienced severe odynophagia resulting from extensive oropharyngeal ulcers due to secondary syphilis. This underscores numerous potential manifestations of syphilis in patients with significant comorbidities [47]. Therefore, clinicians must incorporate sexually transmitted infections in the differential diagnosis of atypical skin lesions. Appropriate tests, such as RPR, VDRL, and TPHA for syphilis, should be performed whenever skin manifestations are of uncertain etiology or are resistant to standard treatment. Patients who are immunosuppressed or have multiple comorbidities might be at higher risk of developing uncharacteristic lesions due to diverse immunopathological processes, and rarer diseases should not be overlooked in these cases.
Conclusions
Lower limb ulcerations often lead to diagnostic and therapeutic difficulties. Sporotrichosis and syphilis frequently imitate other diseases, which may hinder accurate diagnosis. When taking care of immunosuppressed patients or patients with other significant comorbidities, such as diabetes or alcohol dependence, Sporothrix schenckii infection should be included in the differential diagnosis. Whenever skin lesions are resistant to numerous oral and topical drugs, histopathological assessment and mycological investigation, e.g. deep lesion biopsy with a swab, are essential tools in diagnostics. One should consider the possibility of the coexistence of two rare diseases in one patient, especially when they present other immunosuppressive comorbidities.