
Introduction
Immune disorders are a significant challenge to pu-blic health by compromising the body’s ability to effectively ward off pathogens, including viruses. One of the most pressing and global challenges in recent years is the COVID-19 pandemic, caused by the SARS-CoV-2 virus. COVID-19 in unvaccinated patients with inborn errors of immunity (IEI), especially adults, is associated with a high risk of severe disease and death [1]. COVID-19 vaccinations have emerged as a crucial tool in combating the spread of the virus and mitigating its adverse effects on societal health. However, for individuals with immune disorders, such as humoral deficiency or other conditions affecting the immune response, the effectiveness and nature of the post-vaccination response may differ from the general population. Consequently, unverified information regarding the inefficacy and harm of SARS-CoV-2 vaccines has become a concern. Particularly vulnerable are individuals with congenital immunodeficiencies, who were already at a higher risk of infections and severe outcomes before the pandemic [2, 3].
One method for assessing the effectiveness of SARS-CoV-2 vaccinations is the evaluation of post-vaccination antibody levels [4]. Unfortunately, in patients with congenital immunodeficiencies where antibody production is impaired, this method may have limited diagnostic value [5]. Therefore, it was imperative to verify whether and how vaccinations impact not only humoral immunity but also other types of immune responses.
The objective of this study was to conduct a detailed analysis of the immune response following COVID-19 vaccinations in individuals with immune disorders, especially those with humoral deficiency or other significant immunological conditions. Unfortunately, even now, despite the passage of some time since the onset of the pandemic, conspiracy theories regarding the safety and efficacy of SARS-CoV-2 vaccines continue to proliferate. We believe that the results of our study will provide essential information regarding the effectiveness of COVID-19 vaccinations among individuals with immune disorders. The obtained data may contribute to a better understanding of the needs of this patient group and the adjustment of vaccination strategies to achieve maximum protection against the SARS-CoV-2 virus.
Material and methods
In the conducted studies monitoring the immune response in patients with immune disorders, three different tests were used: Anti-SARS-CoV-2 QuantiVac ELISA, SARS-CoV-2 NeutraLISA, and Quan-T-Cell SARS-CoV-2 IGRA (EUROIMMUN). All these tests were performed using the automated sample processing system EUROIMMUN Analyzer I-2P, following the instructions provided in the kit protocols.
Patients
The study was conducted from November 2021 to October 2022. Inclusion criteria included a diagnosis of humoral inborn errors of immunity (hIEI) based on the European Society for Immunodeficiencies (ESID) criteria and obtaining informed consent to participate in the study. The analysis was performed on samples obtained from patients treated at two immunology centres in Bydgoszcz, Poland. All participants were indigenous inhabitants of Central Europe, belonging to the Caucasian race. The study received approval from the Bioethics Committee of the Nicolaus Copernicus University in Torun at Ludwik Rydygier Collegium Medicum in Bydgoszcz (approval no. KB173/20). Detailed patient characteristics are presented in Table 1. Before the sample collection, patients completed a medical questionnaire regarding their medical history, ongoing therapies, and their status concerning COVID-19, including the course of the disease and vaccination details (type of vaccines, number of doses, and vaccination dates). The diagnosis of COVID-19 was based on the result of a confirmatory PCR test on a nasal swab, performed using various methods in different laboratories. The details of the testing methodologies were not the subject of this study, and the patients were assessed based on their self-reported diagnosis in a medical questionnaire.
Table 1
Patient characteristics
Sample collection
Blood was collected from patients in accordance with ethical principles and after obtaining informed consent to participate in the study. For antibody tests, blood was drawn into clot-maintaining tubes. For the IGRA test, blood was collected into tubes containing heparin as an anticoagulant. Fresh blood was divided into stimulation tubes and incubated for 16 hours at 37°C.
Serological tests
The Anti-SARS-CoV-2 QuantiVac ELISA is a test used for the detection and quantitative determination of immunoglobulin G (IgG) antibodies against SARS-CoV-2. In this test, the patient’s serum was incubated with the S1 antigen, which was surface-bound to a microtitre plate. After incubation and washing, IgG antibodies present in the serum were detected using an enzyme conjugated to anti-human antibodies. The addition of an enzyme substrate led to the development of a colour reaction, and its intensity was measured. The resulting reading was reported in binding antibody units per millilitre (BAU/ml) and allowed for the quantitative assessment of IgG antibody levels against the SARS-CoV-2 antigen.
SARS-CoV-2 NeutraLISA is a competitive ELISA test used to evaluate the ability of patient antibodies to neutralize SARS-CoV-2. Neutralizing antibodies have the property of blocking the binding process of SARS-CoV-2 to the ACE2 receptor on the surface of human cells. The method was based on the assumption that in the tested sample, neutralizing antibodies compete with the biotinylated ACE2 receptor for binding sites on the S1 antigen of SARS-CoV-2. If neutralizing antibodies are present in the sample, they hinder further reaction steps, resulting in the absence of a colour reaction after the addition of a substrate. On the other hand, in the absence of neutralizing antibodies, the biotinylated ACE2 receptor binds to the S1 antigen, leading to a colour reaction. The result was reported in percentages, enabling the assessment of the antibodies’ ability to neutralize the virus. The SARS-CoV-2 NeutraLISA assay, used in this study, is a surrogate neutralization test that detects neutralizing antibodies against SARS-CoV-2 by measuring their ability to block the binding of the ACE2 receptor to the viral S1 spike protein. It does not directly measure virus neutralization but provides an indirect assessment of neutralizing antibody activity.
Quan-T-Cell SARS-CoV-2 (IGRA) is a test used to evaluate the cellular immune response activity of patients against the SARS-CoV-2 virus. The test relies on incubating patient blood samples with virus antigens, which are presented to T lymphocytes. If T lymphocytes have had previous contact with virus antigens, they release interferon γ (IFN-γ), which is a marker of cellular immune response activity. The test consists of two stages. In the first stage, freshly drawn blood is incubated with the S1 antigen of SARS-CoV-2. If T lymphocytes have had prior exposure to virus antigens, they release IFN-γ. In the second stage, an ELISA test was performed to measure the quantity of secreted IFN-γ. The result was reported in milli- International Units per millilitre (mIU/ml) and allowed for the assessment of the cellular immune response activity of patients against SARS-CoV-2.
Statistical analysis
The study’s statistical analysis used descriptive statistics due to small sample sizes, including mean, standard deviation, median, minimum, and maximum values to describe antibody levels and immune activity. Despite sample limitations, this approach offered insights into examined parameters. To assess the relationships between the results of the immunological tests, Spearman’s correlation coefficient was applied. Correlations between three parameters were analysed: IgG anti-SARS-CoV-2 concentration (BAU/ml), the percentage of neutralizing antibodies (%), and the level of IFN-γ (mIU/ml). The analysis was conducted separately for the entire study group (n = 63). A p-value of < 0.05 was considered statistically significant. Statistical analyses and data visualizations were performed using IBM SPSS Statistics version 29.0.2.0 and jamovi version 2.3.26.
Results
Patient characteristics
In the study, a group of patients with various humoral immune system disorders was analysed. The study group consisted of 63 patients, with 31 (49.21%) being females and 32 (50.79%) males. The patients were divided into several age groups, with the largest group being patients aged 11 to 18 years (23.81%) and those aged 31 to 40 years (23.81%). In terms of immunological classification, the patients in the study group were categorized into different groups. The largest group consisted of patients diagnosed with common variable immunodeficiency (CVID) under code D83 (38.10%). Other categories included patients with agammaglobulinaemia, IgG subclass deficiencies, other antibody production disorders, and various humoral response disorders. Among them 31.75% had a history of SARS-CoV-2 infection, while 68.25% did not have such a history. 23.81% reported experiencing symptoms of infection, while 7.94% had no symptoms. However, the dataset lacked details regarding the severity of these cases, including hospitalization or ICU admissions, which limits the depth of analysis.
The study was conducted from November 2021 to October 2022, covering the final phase of the fourth wave (Delta), the fifth wave (Omicron BA.1/BA.2), and the sixth wave (Omicron BA.4/BA.5) of the COVID-19 pandemic. Patients included in the study had confirmed SARS-CoV-2 infections during the second wave (5 patients), third wave (6 patients), fourth wave (5 patients), and fifth wave (2 patients) of the pandemic. COVID-19 vaccinations began in Poland in December 2020, and the first patients in our group were vaccinated as early as January 2021, approximately 10 months before the study began.
Regarding COVID-19 vaccination, patients received various types of vaccines, with the most commonly chosen vaccine being Pfizer/BioNTech (84.13%). 44.44% of patients received two vaccine doses, while 50.79% received three doses. The most common period since the last vaccine dose was three quarters (55.56%). However, there was significant variation in the time since the last vaccine dose within this group (Table 1).
The vaccination history of the cohort reflects significant heterogeneity. Patients received different vaccine types and varying numbers of doses, and the intervals between vaccination and serological testing also differed. This diversity is acknowledged as a limitation of the study, but it provides a more realistic representation of the varied vaccination schedules encountered in clinical practice. Future analyses could explore how these factors influence immune responses to SARS-CoV-2 vaccines.
Serological test results
The serological analysis results are presented in Table 2 and Figure 1. The serological test results revealed significant differences in the levels of IgG anti-SARS-CoV-2 antibodies, neutralizing IgG antibodies (NEUT IgG), and IFN-γ concentration based on the patients’ immunological diagnoses. Patients with various immunological disorders exhibited diverse immunological responses to SARS-CoV-2 infection and vaccination.
Table 2
Comparison of serological parameters among patient groups
Fig. 1
Comparison of serological test results across different diagnoses, IgG antibody concentration against SARS-CoV-2 (A), percentage of neutralizing antibodies (B), and interferon γ concentration (C)
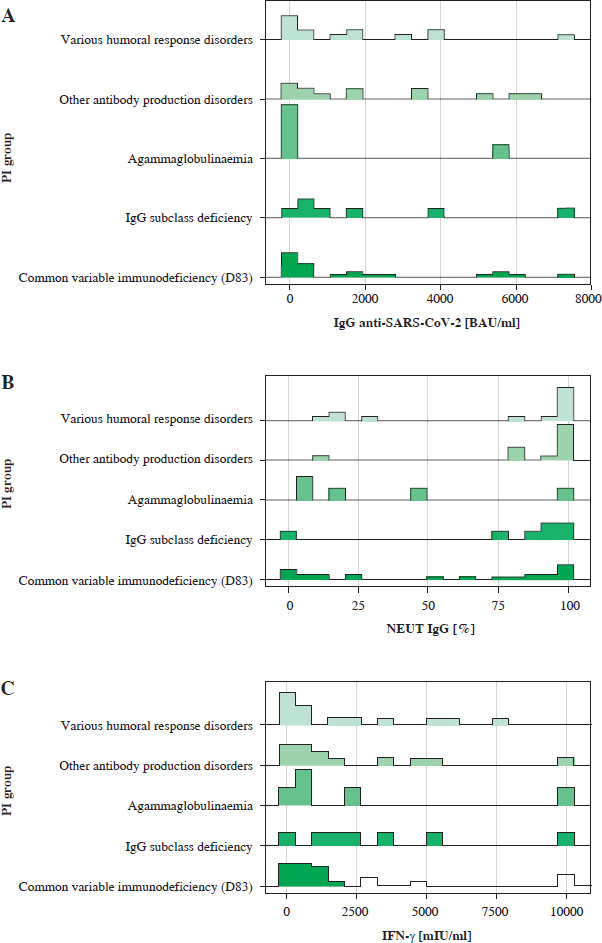
IgG anti-SARS-CoV-2. In terms of IgG anti-SARS-CoV-2 antibody levels, the results show variation among patients with different immunological diagnoses. The highest mean antibody level was observed in patients with other antibody production disorders (2324.8 BAU/ml) and IgG subclass deficiency (2059.4 BAU/ml). Conversely, patients diagnosed with agammaglobulinaemia exhibited lower mean antibody levels (1124.6 BAU/ml). Various humoral response disorders had an intermediate level (1711.0 BAU/ml), and patients with common variable immunodeficiency had a mean level of 1756.0 BAU/ml. It is worth noting that the lowest IgG anti-SARS-CoV-2 antibody levels were observed in patients with agammaglobulinaemia, with a wide confidence interval, potentially stemming from the small number of patients in this category. Moreover, agammaglobulinaemia and IgG subclass deficiency exhibited a high degree of variability, as suggested by their 95% confidence intervals.
Neutralizing IgG antibodies. Regarding neutralizing IgG antibodies (NEUT IgG [%]), patients with other antibody production disorders showed the highest mean level (88.5%), while patients with agammaglobulinaemia had the lowest mean level (35.6%). Various humoral response disorders had an intermediate level (74.6%). Notably, in the case of agammaglobulinaemia, the confidence interval again showed variability in the results. The significant result (p = 0.027) suggests differences in the neutralizing capacity of antibodies against the SARS-CoV-2 virus based on the type of immunological disorder.
IFN-γ concentration. Concerning IFN-γ concentration, patients diagnosed with IgG subclass deficiency exhibited the highest mean concentration (3502.5 mIU/ml). Subsequently, patients with other antibody production disorders (2275.6 mIU/ml) and CVID (2174.0 mIU/ml) presented similar mean concentrations. Various humoral response disorders had a lower mean concentration (1986.1 mIU/ml), and patients with agammaglobulinaemia exhibited a mean concentration of 275.9 mIU/ml.
These comparisons provide a general overview of the differences in serological parameters between patient groups. The results of the serological parameter analysis indicate significant differences in the immunological response of patients to SARS-CoV-2 antigen exposure based on their immunological diagnoses. Patients with agammaglobulinaemia tended to exhibit lower levels of IgG antibodies and neutralizing IgG antibodies compared to other patients. Comparing the IFN-γ levels in patients with agammaglobulinaemia to other groups of immunodeficient patients, it was observed that the cellular response, assessed based on interferon concentration, was quite robust. Only patients with IgG subclass deficiency exhibited higher IFN levels compared to the agammaglobulinaemia group. Patients with IgG subclass deficiency tended to have higher IFN-γ levels (3502.5 mIU/ml vs. 2675.9 mIU/ml). However, it is important to note that these comparisons are based on averaged data, and individual variations within each group may exist. Other factors that could potentially influence the results include the time since exposure to SARS-CoV-2 antigen, the number of vaccine doses received, the type of vaccine administered, and prior infection. These observations suggest that specific immunological disorders may influence the immunological response of patients to COVID-19 vaccinations. Therefore, while these comparisons provide valuable insights, further analysis considering these factors is necessary to fully understand the impact on serological parameters in each patient group.
For the purpose of facilitating the characterization and comparisons within the different diagnostic groups, several categories were introduced to provide a clearer picture. Firstly, the age variable was divided into two categories, adults (> 18 years old) and children (< 18 years old), acknowledging the potential age-related differences in the immune response. This division allows for a better understanding of how different age groups may exhibit varying serologic profiles. In terms of IgG anti-SARS-CoV-2 concentration (BAU/ml), a categorization was established to differentiate between low (below 200 BAU/ml) and high. This categorization helps identify individuals with a potentially weaker immune response (low concentration) versus those with a stronger response (high concentration). It is worth noting that this division enables a more comprehensive analysis of the IgG antibody levels and their potential implications in immune protection. The proposed threshold of 200 BAU/ml, used to classify weaker and stronger immune responses, remains a contentious issue. While our findings suggest differences in immune responses above and below this threshold, there is no global consensus on its validity as a correlate of protection (CoP). As highlighted by recent studies [6-9], CoPs likely vary among immunodeficient subgroups. Our study reinforces the need for further research to define CoPs tailored to specific immunological disorders.
Another important aspect assessed in the study was the presence of neutralizing antibodies against SARS-CoV-2, which were categorized as being either above or below the 50% threshold. This distinction is crucial since neutralizing antibodies play an important role in preventing viral entry into host cells, and their presence above or below the defined threshold provides insights into the effectiveness of the immune response. The 50% neutralization threshold was chosen arbitrarily for categorization purposes, as there is no definitive evidence that this level of neutralizing antibodies guarantees full protection against infection, particularly in this patient group. Lastly, the cellular response, specifically the IFN-γ concentration, was categorized as positive or negative based on a predefined cut-off value of 200 mIU/ml. This classification helps determine whether individuals exhibit a robust humoral response, as indicated by a positive IFN-γ concentration, or a potentially impaired response, reflected by a negative result. By employing these categories, the analysis aims to enhance the interpretation of the serologic data by considering various factors that might influence the immune response. It provides a more nuanced understanding of the differences and similarities within and between the diagnostic groups, shedding light on important aspects of the immune profiles observed in the study population.
Common variable immunodeficiency
The CVID group comprised 24 individuals, with 10 females and 14 males. They received various vaccine types and doses. Nearly half (45.8%) had a history of SARS-CoV-2 infection. Most (62.5%) had high IgG anti-SARS-CoV-2 antibody levels, and over half (54.2%) had neutralizing antibody levels exceeding 50%. A substantial majority (83.3%) exhibited a positive post-vaccination interferon response, indicating retained immune function.
Regarding SARS-CoV-2 infection, among children with CVID, 4 individuals tested negative, while 2 tested positive. In the adult group, 10 individuals tested negative, and 9 tested positive for SARS-CoV-2 infection. When considering the vaccine name, no individuals in the children’s group received the AstraZeneca, Johnson & Johnson, Moderna, or unspecified vaccines. However, 6 children received the Pfizer/BioNTech vaccine. In the adult group, 1 individual received the AstraZeneca vaccine, 3 received the AstraZeneca vaccine (possible duplicate entry), 1 received the Johnson & Johnson vaccine, 1 received the Moderna vaccine, and 1 received an unspecified vaccine. Additionally, 12 adults received the Pfizer/BioNTech vaccine. Regarding the time from the last vaccination (measured in quarters), among children with CVID, 4 individuals were in the first quarter, 2 were in the second quarter, and there were no individuals in the third or fifth quarters. In the adult group, 10 individuals were in the first quarter, 4 were in the second quarter, 3 were in the third quarter, and 1 was in the fifth quarter. Table 3 presents a comparison of post-vaccination immune responses and reactivity among individuals with different immunological disorders, highlighting variations in IgG levels, neutralizing antibodies, and interferon responses. Regarding the IgG anti-SARS-CoV-2 concentration, it can be observed that a higher proportion of adults (44.0%) had a high concentration of IgG antibodies compared to children (16.0%), where the majority had a low concentration (32.0%). In terms of neutralizing antibodies against SARS-CoV-2, a higher percentage of adults (40.0%) had an antibody level above 50%, indicating a more robust immune response, while only 8.0% of children reached this threshold. Furthermore, the analysis of the humoral response, as indicated by IFN-γ concentration, revealed that a greater proportion of adults (60.0%) exhibited a positive response, suggesting a more active immune reaction. In contrast, no children in the sample showed a negative response, while 24.0% exhibited a positive response. These comparisons highlight differences in serological parameters between children and adults with CVID. Adults generally demonstrate higher levels of IgG antibodies, a higher percentage of neutralizing antibodies, and a more pronounced humoral response compared to children. These findings suggest potential age-related variations in the immune response to SARS-CoV-2 infection among individuals with CVID.
Table 3
Comparison of post-vaccination immune responses and reactivity in disorder groups
Agammaglobulinaemia
The analysis of the immunological response in patients diagnosed with agammaglobulinaemia (including D80.0 and D80.1) reveals distinctive features in their reaction to SARS-CoV-2 infection and vaccination. The study group consisted of five adult patients, including two females and three males. All patients received SARS-CoV-2 vaccines, with one person receiving the AstraZeneca vaccine and the remaining four receiving the Pfizer/BioNTech vaccine. Among the examined patients, two received two vaccine doses, while three received three doses. Neutralizing antibodies against SARS-CoV-2 were below 50% in four patients, indicating limited ability to neutralize the virus. One patient exhibited neutralizing antibody levels exceeding 50%. Importantly, all studied patients displayed a positive interferon response following SARS-CoV-2 vaccination.
The immunological response in patients with agammaglobulinaemia had several key characteristics. Only one-fifth of the patients with agammaglobulinaemia (20.0%) had a history of symptomatic SARS-CoV-2 infection. All patients with agammaglobulinaemia exhibited low concentrations of IgG anti-SARS-CoV-2 antibodies, consistent with the nature of their diagnosis. In the group of patients with agammaglobulinaemia (n = 5), the anti-SARS-CoV-2 IgG antibody levels showed high variability. Four out of the five results (4.73; 11.76; 14.26; 46.80) fell within a low range, which corresponds to the limited or absent production of immunoglobulins characteristic of this condition. However, one result (5545.60) is a clear outlier. A possible explanation for this phenomenon is that the blood sample was taken shortly after the administration of immunoglobulin preparations (IVIG/SCIG), which might have resulted in the passive transfer of antibodies contained in the preparation rather than reflecting the patient’s endogenous production. Additionally, in this patient (a 47-year-old male), the blood sample was taken 5 weeks after receiving the third dose of the Pfizer/BioNTech vaccine, corresponding to the peak level of antibodies after vaccination. It is noteworthy that one patient had neutralizing antibody levels exceeding 50%, suggesting a certain ability to neutralize the virus despite the absence of conventional IgG antibodies. All examined patients demonstrated a positive interferon response following SARS-CoV-2 vaccination, indicating preserved functions of the immune system in producing interferon in response to the virus antigen.
The conclusions drawn from this analysis suggest that patients with agammaglobulinaemia exhibit limited capacity to produce conventional IgG antibodies and have a low incidence of symptomatic SARS-CoV-2 infection. However, the presence of neutralizing antibodies and a positive interferon response may indicate a certain level of protection against the virus. Further research is necessary to gain a better understanding of the mechanisms of the immunological response in patients with agammaglobulinaemia in the context of SARS-CoV-2.
IgG subclass deficiency
This subgroup comprised seven patients, with five females and two males. All patients received SARS-CoV-2 vaccines, with one patient receiving the Johnson & Johnson vaccine and the remaining six receiving the Pfizer/BioNTech vaccine. Among them, one received one vaccine dose, one received two doses, and five received three doses, with varying intervals since the third dose. Most patients (71.4%) had no prior SARS-CoV-2 infection history. Despite the subclass deficiency, 85.7% of patients displayed high levels of IgG anti-SARS-CoV-2 antibodies. Similarly, 85.7% showed neutralizing antibody levels exceeding 50%, indicating effective neutralization. All patients exhibited a positive interferon response after vaccination, suggesting maintained immune functionality.
Other antibody production disorders
Our analysis included 13 patients diagnosed with other antibody production disorders (including D80.8), comprising eight females and five males. All received SARS-CoV-2 vaccines, with two receiving Moderna and the rest Pfizer/BioNTech. Five received two doses, and eight received three doses, with various post-third dose intervals. Most (69.2%) had no prior infection history. Despite their disorders, 76.9% exhibited high IgG anti-SARS-CoV-2 antibody levels, and 92.3% had neutralizing antibody levels exceeding 50%. A significant majority (76.9%) showed a positive post-vaccination interferon response, indicating preserved immune functionality.
Various humoral response disorders
This group included 14 individuals diagnosed with various humoral response disorders. Most (57.1%) received two Pfizer/BioNTech vaccine doses, and 35.7% received three doses. Over two-thirds (64.3%) had high IgG anti-SARS-CoV-2 antibody levels, and a similar proportion (71.4%) had neutralizing antibody levels exceeding 50%. Additionally, 64.3% showed a positive interferon response following vaccination, suggesting preserved immune functionality.
Correlations between immunological parameters
The analysis revealed a significant, moderate positive correlation between the percentage of neutralizing antibodies and the level of IFN-γ (rho = 0.456, p < 0.001). Furthermore, the percentage of neutralizing antibodies showed a strong correlation with the concentration of IgG anti-SARS-CoV-2 (rho = 0.599, p < 0.001). However, no significant correlation was found between the level of IgG anti-SARS-CoV-2 and IFN-γ (rho = 0.073, p = 0.568), nor between the classification of patients and the individual immunological parameters.
Discussion
Patients with primary immunodeficiencies are at an increased risk not only for infections but also for more severe disease outcomes [1-3]. Consequently, this patient group had been implementing protective measures even before the onset of the pandemic. The introduction of remote visits further allowed for a reduction in direct contact with healthcare services. In Poland, patients with primary immunodeficiencies qualifying for immunoglobulin substitution are scheduled separately from other patients, maintaining a spatial and temporal distance regimen. Home deliveries of medicines were also implemented, which also contributed to protecting patients against infections. These measures resulted in 68% of the analysed patients having no documented SARS-CoV-2 infection. Studies on COVID-19 in patients with primary immunodeficiencies mainly focus on analyses where the infection occurred. However, there are limited data determining the frequency of SARS-CoV-2 infection in the CVID population. Similar findings were reported by Napiórkowska-Baran et al., analysing patients from four reference immunological centres for adults. The study found a nearly 30% infection rate with the SARS-CoV-2 virus [10].
The introduction of COVID-19 vaccinations has played a crucial role in further protecting patients with IEI from severe disease outcomes. Given their heightened susceptibility to infections and complications, vaccination has been a key preventive strategy in reducing the risk of hospitalization, intensive care unit admissions, and mortality in this vulnerable group. Recent studies, including the USIDNET report [11], have demonstrated that vaccination significantly lowers the rates of severe COVID-19 among patients with inborn errors of immunity, with vaccinated individuals experiencing a lower incidence of hospitalization (9.3% vs. 24.4%, p < 0.001) and ICU admissions (2.8% vs. 7.6%, p = 0.013) compared to their unvaccinated counterparts. The authors of the publication demonstrated that COVID-19 vaccination in patients with inborn errors of immunity exhibits a high safety and efficacy profile. Among the 806 vaccinated patients, only 17 required medical consultation due to vaccine-related complications, with a single case of hospitalization reported due to symptomatic anaemia. The study findings confirm that the benefits of vaccination, including reduced disease severity and improved clinical outcomes, substantially outweigh the potential risks of adverse effects [11].
Among the vaccinated patients in our group, the most commonly received vaccine was Pfizer/BioNTech (82.8%). This was in accordance with recommendations suggesting mRNA vaccines for patients with primary immunodeficiencies, deemed safe and characterized by higher efficacy [12]. Currently, the European Society for Immunodeficiencies recommends that patients with primary immunodeficiencies receive any available COVID-19 vaccine, provided they are not live vaccines [13].
Patients with primary immunodeficiencies exhibit significant diversity. Variability in symptoms occurs not only based on the type of identified deficiency (cellular/humoral/complement system disorders, among others), but also among patients with the same disease entity, highlighting differences in clinical manifestation. A notable example is CVID, a group of disorders with a similar phenotype but distinct genetic backgrounds [14]. Therefore, it is crucial to determine not only whether a post-vaccination response in cellular immunity exists but also whether it may differ among patients with primary immunodeficiencies, not only within the entire group but also among specific disease entities.
Another challenge is that the post-vaccination response is commonly assessed in terms of specific antibody production [15, 16]. The COVID-19 pandemic necessitated a shift in the approach to evaluating post-vaccination responses, emphasizing cellular immunity as a crucial factor in combating the virus [17, 18]. Cellular immunity can be assessed by determining specific RBD+ IgG+ memory B lymphocytes using flow cytometry, but this test is available only in selected highly specialized centres [19]. A simpler and more accessible test involves measuring IFN-γ levels after in vitro stimulation with SARS-CoV-2- specific peptides [20]. In the literature, isolated publications can be found regarding the application of this method in patients with primary immunodeficiencies [21, 22]. This is significant, as the majority of primary immunodeficiencies involve humoral immune deficiencies [23], and cellular immunity plays a crucial role in the response to pathogens in these patients.
Recent studies provide further insights into the complex dynamics of immune responses in patients with primary immunodeficiencies, highlighting both the challenges and potential strategies for optimizing vaccine efficacy in this vulnerable population. Gupta et al. [24] demonstrated substantial variability in both humoral and cellular immune responses among patients with primary antibody deficiencies following COVID-19 vaccination. While these patients exhibited lower levels of specific anti-SARS-CoV-2 IgG antibodies, their cellular immunity, particularly T-cell-mediated responses, remained remarkably robust. This observation underscores the critical role of T-cell responses in compensating for impaired humoral immunity in primary immunodeficiency patients, especially in the context of SARS-CoV-2 infection and vaccination. The study further emphasizes the heterogeneity of responses, even within subgroups of patients with similar diagnoses, suggesting the need for individualized approaches to vaccination [24]. Vossen et al. [25] provided critical evidence for the benefits of administering a third dose of COVID-19 vaccines to patients with inborn errors of immunity, including those with mannose-binding lectin deficiencies. The third dose significantly improved both humoral responses, as measured by neutralizing antibody levels, and cellular responses, including T-cell activation and IFN-γ production. These findings align with our observations, where patients receiving three doses demonstrated higher neutralizing antibody levels and a more pronounced cellular immune response, as measured by IFN-γ concentrations, compared to those receiving only two doses. This underscores the importance of tailored vaccination schedules in achieving optimal protection for individuals with primary immunodeficiencies. Long-term monitoring of immune responses in primary immunodeficiency patients is another critical area of focus. Hurme et al. [26] emphasized that the durability of vaccine-induced immunity varies significantly over time, particularly in patients with antibody deficiencies. Their findings support the necessity of regular serological and cellular immunity assessments to evaluate the effectiveness of vaccination and guide subsequent booster strategies. Consistent with our data, they observed that antibody titres and neutralizing activity decreased over time, highlighting the potential need for periodic booster doses to sustain immunity in this population.
Murray et al. [27] found that up to 89% of individuals with primary immunodeficiencies had interferon-gamma levels exceeding the reference range after stimulation with SARS-CoV-2 peptides following primary vaccination, compared to 99% of healthy individuals in the control group and 76% of those with secondary immunodeficiencies. Although IFN-γ levels were significantly lower than in healthy individuals, they were notably higher than in patients with secondary immunodeficiencies, highlighting the critical role of cellular immunity in this patient group. Following a booster dose, a statistically significant increase in IFN-γ production was observed (p = 0.0156), indicating the potential of booster doses to further enhance cellular immunity in primary immunodeficiency patients. Additionally, detectable levels of specific antibodies against spike proteins were found in 100% of healthy individuals in the control group, 70% of primary immunodeficiency patients, and 64% of individuals with secondary immunodeficiencies after primary vaccination. The study also highlighted the lower prevalence and reduced levels of neutralizing antibodies in primary immunodeficiency patients, further underscoring the importance of cellular responses in mitigating the risk of severe COVID-19 in this population. The authors emphasized that the whole-blood IGRA test is an accurate, simple, and reliable tool that can be easily adapted to measure cellular responses to COVID-19, even in patients with primary immunodeficiencies. In the group of patients with primary immunodeficiencies, those with CVID and agammaglobulinaemia constituted the majority, while in our study, the CVID group was the largest, with patients with agammaglobulinaemia comprising only 8% of the study group (vs. 22%). The authors emphasized that whole blood IGRA is a very accurate, simple, and robust test that can be easily adapted to measure the cellular response to COVID-19, even in patients with primary immunodeficiencies. Clinical evaluation of immunodeficiency and confirmed assessment of vaccine response can be valuable tools in estimating the risk of COVID-19 and identifying individuals with immunodeficiencies who may benefit from enhanced vaccination schedules [27].
The observed correlation between the percentage of neutralizing antibodies and the level of IFN-γ may indicate a link between the humoral and cellular immune responses in the studied patient population. The strong positive correlation between the total IgG anti-SARS-CoV-2 concentration and the percentage of neutralizing antibodies suggests that the amount of specific antibodies does not always directly correlate with their neutralizing properties. The lack of a significant correlation between the IgG level and IFN-γ may reflect the complex interaction between humoral and cellular immunity.
These findings collectively emphasize the critical importance of adopting individualized, multifaceted approaches to vaccination in patients with primary immunodeficiencies. Tailored vaccination regimens, combined with regular monitoring of both humoral and cellular responses and potential adjunctive therapies, hold promise for improving protection against SARS-CoV-2 in this vulnerable population.
A limitation of our study was the absence of a control group. Given the severe consequences of SARS-CoV-2 infection in patients with immune deficiencies, we prioritized enrolling as many patients with IEIs as possible. Another limitation is that the presence of antibodies in patients could be attributed to various factors, including prior SARS-CoV-2 infection (both symptomatic and asymptomatic, confirmed or not), vaccination, and the use of antibody substitution therapies, which are commonly administered to patients in our study group. The antibodies present in immunoglobulin preparations may also result from natural infection and/or a post-vaccination immune response [28]. During the analysis of the patient samples, we conducted studies on one of the antibody replacement preparations, with IgG antibody levels against SARS-CoV-2 ranging from 150 to 200 BAU/ml.
Conclusions
Our study focused on analysing the immunological response of patients with immune disorders following COVID-19 vaccination. Utilizing various serological tests, we identified significant variations in immune responses depending on the type of immune disorder. Patients with agammaglobulinaemia demonstrated the ability to neutralize the virus despite low levels of IgG antibodies, while patients with IgG subclass deficiency exhibited robust antibody responses and effective neutralization. Our findings may have significant implications for tailoring vaccination strategies for this vulnerable patient group.